

"From triage to discharge: a user?s guide to navigating hospitals" by Michael Vagg, Clinical Senior Lecturer at Deakin University School of Medicine & Pain Specialist, licensed under CC BY-ND 4.0
Australia's public hospital system has been consistently ranked among the best in the world. But whether it's an emergency or a planned admission, going to hospital can be anxiety-inducing ? not knowing where you're heading or who will be looking after you.
Here's a cheat sheet to guide you.
I've worked in and around hospitals for most of my adult life ? from inflatable military tents in the scrub, to multi-million dollar towers in the inner city. The one thing they all have in common are inpatients: the people who occupy beds.
Then there are outpatients, who are outside the hospital except when they are seeing a practitioner for care.
How you get there
You get into a hospital either by choice (elective admission) or by necessity (acute admission).
Most acute admissions occur via the hospital emergency department (ED), where you turn up with what seems like it may be a serious problem to find out whether you need to worry or not.
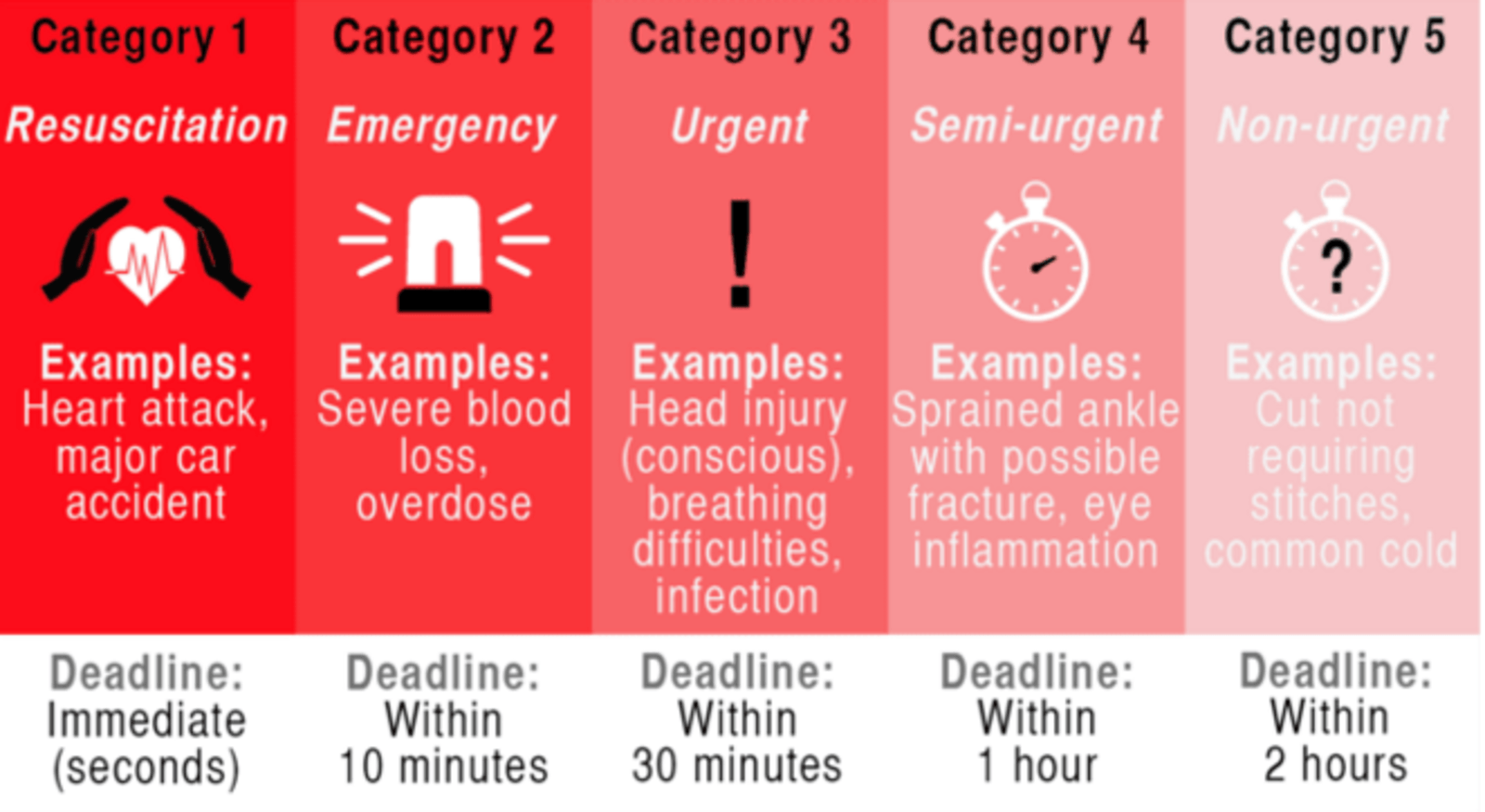
One element of EDs which can cause frustration is the triage assessment. This idea goes back to the Napoleonic wars, and is a systematic way of ensuring the sickest patients ? such as those who have had a heart attack or stroke ? get seen first.
Patients arriving by ambulance are usually triaged by the paramedics en route and seriously injured or unwell people will arrive to a waiting resuscitation team.
There is a national standard for triage categories, with attached key performance indicators:
Experienced ED nurses do the triage assessments, and can be trusted to know a truly unwell patient when they see one. Noisy, crying infants are generally not as much of a concern as quiet, listless ones, for example. For the many annoyed-but-coping people who have to wait longer than they think they should, there are a few lives saved by astute triage nurses who spot subtle but serious warning signs and expedite care though the patient may not seem too bad at the time.
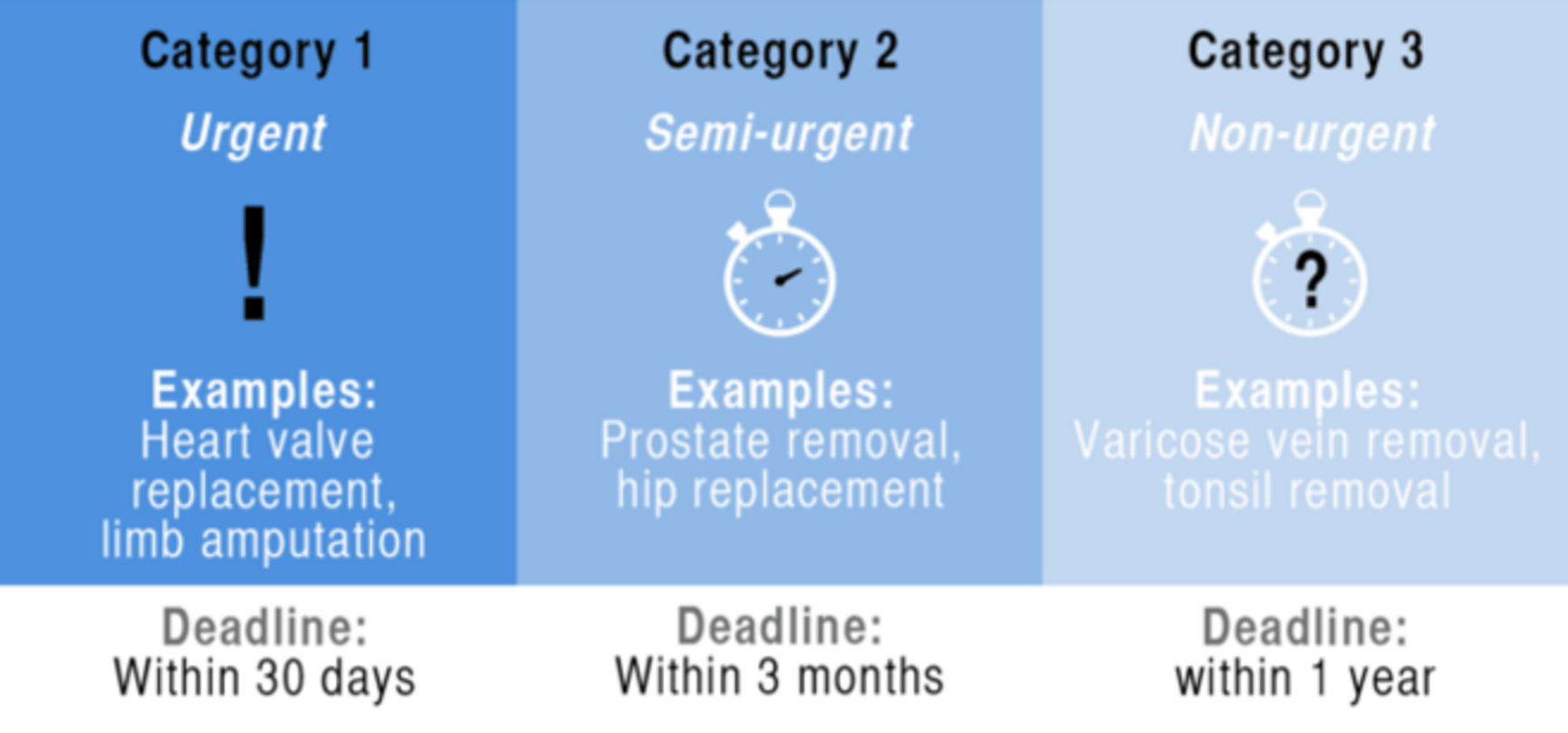
Elective admissions are planned admissions for assessment or treatment. Examples include joint replacement surgery, cancer treatment with chemotherapy or radiotherapy, or inpatient assessment of a challenging diagnosis.
Elective admissions most often arise from outpatient consultations. Your GP refers to the relevant outpatient service for an assessment or treatment. If you need a procedure or inpatient treatment, you go on the much-discussed waiting list for treatment.
You will be assigned some type of urgency rating, the details which vary a little state by state:
Who looks after you?
Once you make it into the hospital you get sent to a ward. Each ward is like a little community with a cast of regular staff and one or two areas of particular expertise.
The key person on any ward is the nurse in charge, confusingly known in some hospitals as the unit nurse manager, the nurse unit manager, or occasionally simply the team leader. This nurse is responsible for the daily myriad of tasks that make a ward function. In my view, the vibe of a ward also tends to take on the personality of its leader over time. Some will be free-wheeling and innovative, others will be super-efficient and focused.
The nurse unit manager (NUM) is supported by a number of associates, with one of the ANUMs in charge of every shift around the clock.
Doctors in a hospital are organised into units. Each unit generally consists of one or more senior specialists, known as consultants or visiting medical specialists, grouped according to specialty or a particular group of patients. The consultants in a unit may work full-time for the hospital for a salary (a staff specialist) or be there for part of the week (hence the title "visiting").
The lynchpin of a medical unit is the registrar, a junior doctor who will usually be undergoing training in the specialty of the unit. The registrar has direct responsibility for the day-to-day care of the unit?s inpatients and outpatients, and normally works full-time in this role.
The registrar is supported by one or more hospital medical officers (HMOs) who are doctors within a couple of years of graduating. HMOs rotate through the various units every couple of months to gain breadth of experience in a supervised setting. In general, if you want something done in a big hospital, the HMOs know the quickest and most effective way to get that to happen.
Each unit has a variable roster of allied health professionals depending on its purpose and resources. Allied health professionals include clinicians such as physiotherapists, occupational therapists, psychologists, speech therapists, dietitians and social workers.
Then where do you go?
Allied health professionals come into their own in sub-acute hospitals, which concentrate on areas such as rehabilitation, aged care and palliative care. These facilities may be co-located with an acute care hospital or on another campus entirely. Most of the inpatients at sub-acute hospitals have come from acute hospitals, but many will also have been admitted from home.
If you are heading home, you may need ongoing support from a "home hospital" type service, which is a major innovation in the last decade. Lengthy courses of antibiotics or prolonged wound healing would once have left otherwise well people stuck in hospital, but some services can now be provided at home by nurses who visit once or twice a day.
As well as nursing care, hospitals liaise with general practitioners to continue your medical care and community groups who can provide help with meals, shopping, housework and personal care while you are getting back to full strength again.
The structure and workings of hospitals have changed enormously over the course of my 20-odd years in medicine. Once we thought of hospitals as places to get cured or die, they now cater to all eventualities in between.

 Reply With Quote
Reply With Quote



 Hopefully it isn't anything bad
Hopefully it isn't anything bad  I had to have the scope because of 24/7 abdominal pain and IBS, but I don't get any cramps luckily. The colonoscopy came back completely normal for me though.
I had to have the scope because of 24/7 abdominal pain and IBS, but I don't get any cramps luckily. The colonoscopy came back completely normal for me though.